This is the old United Nations University website. Visit the new site at http://unu.edu
![]()
![]()
![]()
Methods
Results
Discussion
References
Jinkou Zhao, Hua Wang, Jun Ge, Qinlan Zhang, Xiping Huan, Li Shang, Renjie Pan, and Frits van der Haar
Jinkou Zhao, Hua Wang, Qinlan Zhang, Xiping Huan, and Li Shang are affiliated with the Jiangsu Provincial Center for Public Health and Disease Control in Nanjing, People’s Republic of China. Jun Ge is affiliated with the Office of Endemic Disease Control, Jiangsu Provincial Government in Nanjing. Renjie Pan is affiliated with the Jiangsu Provincial Salt Company in Nanjing, and Frits van der Haar is affiliated with the Department of International Health in the Rollins School of Public Health at Emory University in Atlanta, Georgia, USA.
Mention of the names of firms and commercial products does not imply endorsement by the United Nations University.
Abstract
To assess the iodine-deficiency disorder status in nine counties of Jiangsu Province, China, where salt iodization was initiated in 1985, a special verification survey was conducted in 1997 by a provincial multisectoral team. Results obtained by regular monitoring of counties indicated that the goitre rate in schoolchildren had progressively decreased from 41.9% in 1983 to 3.9% in 1997, while the median urinary iodine concentrations of the population had remained above 100 mg/L since 1985. More than 90% of the edible salt supplied to households had been iodized at ³ 20 mg I/kg during the previous five years. The data obtained by provincial verification confirmed the county findings of: ³ 90% adequate iodized salt in households, < 5% goitre rate in schoolchildren, and adequate urinary iodine excretions. The provincial team also considered the established mechanisms for salt iodization and supply and iodine information management potentially sustainable. The high variability of the iodine content of household salt indicates that improved quality assurance of iodized salt at production and continued monitoring of population iodine indicators are needed.
Introduction
Iodine deficiency is the leading cause of preventable intellectual deficit worldwide, with 1.6 billion people globally at risk [1]. The prevention of iodine-deficiency disorders received a major impetus at the 1990 United Nations Global Summit for Children from the call by world leaders for its virtual elimination by the year 2000 [2]. Following recommended policy [3], salt iodization has been started in many countries, and almost all have passed legislation to assure its implementation. UNICEF estimated that by 1997 nearly 60% of all the edible salt produced in the world was iodized [4].
In Jiangsu, a province in China with 70 million inhabitants, endemic goitre and mental retardation have long been recognized as a public health problem. Provincial surveys of iodine -deficiency indicators during the early 1980s showed an average prevalence of goitre of 25.5% among 7- to 14-year-old schoolchildren, a mean urinary iodine concentration in the population of 76 mg/L, and an average drinking water iodine content of 6.6 mg/L [5]. Nine of the 75 counties of the province, Gaoqun, Jiangning, Jiangpu, Jintan, Jurong, Lishui, Liyang, Luhe, and Xuyi, were most severely affected, with an overall total goitre prevalence of 41.9% in schoolchildren in 1983. In 1985, before its introduction throughout the province, salt iodization was initiated in these counties, and by 1997 the policy had been in place for more than 10 years.
Since 1993, when the Chinese government proclaimed the national goal of elimination of iodine-deficiency disorders by the year 2000, a substantial amount of human and financial resources has been mobilized throughout the country. Universal salt iodization, requiring 50 mg I/kg salt at production, was started in Jiangsu Province in 1995. The supply and quality of iodized salt have been improved continually by the salt industry, and provincial data indicate that 90% or more of the population have had access to iodized salt since 1996 [6].
To follow the progress being made towards elimination of iodine- deficiency disorders in all the counties of Jiangsu Province, a surveillance system was devised based on provincial investigation of iodine- deficiency disorder indicators every two years and continuous monitoring of the iodine content in salt. According to national guidelines, all counties collect 25 salt samples for titration monthly from salt factories and households, and quarterly from retail outlets. Each month the iodine content of salt samples obtained at the factory, retail, and household levels is checked using rapid test kits.
In 1997 government officials and management personnel from the provincial health and salt sectors formed a special evaluation team to assess the salt and iodine status of the population in the nine counties of Jiangsu Province most at risk. The overall aim was to determine whether there was sufficient evidence that virtual elimination of iodine-deficiency disorders had been achieved in these nine counties, based on criteria recommended by the World Health Organization/UNICEF/International Council for the Control of Iodine-Deficiency Disorders [7].
Review of existing data
The provincial team inspected the monitoring records from each county and reviewed the data on total goitre rates and urinary iodine concentrations among schoolchildren and salt iodine contents at salt factories, retailers, and households for the previous five years.
Self-evaluation by county
County officials divided each township into five areas that served as primary sampling units. The population of each primary sampling unit was listed alphabetically, and 30 clusters were selected proportionately to population size [7]. One elementary school was randomly selected per cluster, and in each school, 40 pupils aged 8 to 10 years were selected at random from the attendance roster for palpation of thyroid size, 25 pupils for collection of salt samples brought from home, and 12 pupils for casual collection of urine samples.
Verification by the provincial team
Each county was divided into five areas of approximately equal size, and two elementary schools were randomly selected in each area. In each school, 40 pupils aged 8 to 10 years were selected at random from the attendance roster for palpation of thyroid size and ultrasonography, and 12 pupils for casual collection of urine samples. In each area, 25 pupils were selected to bring a salt sample from home for iodine titration.
Thyroid size determination
County health professionals palpated the thyroid gland and classified the grade of goitre according to the WHO/UNICEF/ICCIDD description [7]. For verification, an experienced physician obtained an ultrasonogram of the thyroid gland with a portable ultrasound unit equipped with a 7.5-MHz linear array transducer (AKHO, Canada). The depth (d), width (w), and length (1) of each lobe in millimetres were obtained from longitudinal and transverse scans, and the volume of the lobe was calculated by the formula [8]:
V (ml) = 0.479 × d × w × 1 × 1/1,000
The thyroid volume was the sum of the volumes of both lobes without including the volume of the isthmus. Thyroid size was classified according to age standards [10].
Laboratory methods
Urinary iodine was analysed by the acid-digestion method [9]. The iodine content in salt samples was obtained by titration [101. The urine and salt samples from the county self-evaluation surveys were analysed in county laboratories, which are accredited by the provincial laboratory. All iodine analyses for the verification survey were done by the provincial laboratory, which is under regular quality surveillance by the Chinese Academy of Preventive Medicine in Beijing and the National Institute of Iodine- Deficiency Disorders in Harbin. Urinary iodine analysis of 18 blinded control samples at three levels by the provincial laboratory did not demonstrate bias compared with the results from the reference laboratories. The precision of these determinations was 2.4%.
Data analysis
All field survey and laboratory data were analysed with Epi Info 6.04. The total goitre rate according to palpation was calculated as the proportion of pupils with grade 1 or 2 goitre. The total goitre rate according to ultrasonography was calculated as the proportion of pupils with thyroid volume above the age-specific reference [11]. Because of their skewed distributions, the median was used to measure the central tendency of urinary iodine concentrations.
A county was declared to be free of iodine- deficiency disorders if ³90% of households had access to adequately iodized salt during the last five years; the median urinary iodine concentration of the population was above 100 mg/L; and a sustainable mechanism for monitoring salt iodine content and iodine-deficiency disorders had been established. For the purpose of this survey, salt samples from households with an iodine content above 20 mg/kg were classified as adequate.
County monitoring records
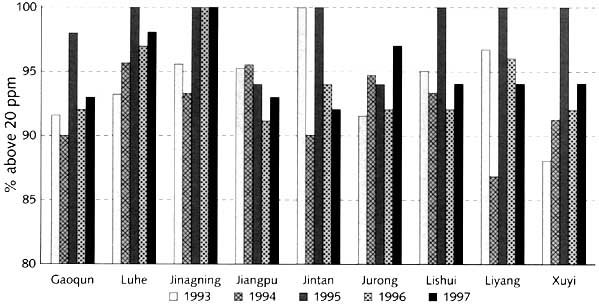
Figure 1 shows the percentage of household salt samples containing adequate iodine from 1993 to 1997, obtained from review of county monitoring records. In 2 of 45 possible occurrences (once each in 1993 and 1994), the adequacy was below 90%. Overall, however, in each county ³90% of the household salt samples had adequate iodine according to titration during the five-year period.
FIG. 1. Adequacy of iodized salt in households in nine counties during 1993-97
The results obtained by provincial review of the county’s urinary iodine and total goitre monitoring since 1983 are shown in table 1. The median urinary iodine concentrations exceeded 100 mg/L in all counties from 1985 onwards, and the total goitre rate declined to below 20% in 1988-1989, below 10% in 1995, and below 5% in 1997 (fig. 2).
County self-evaluation
The self-evaluation results obtained by the counties are presented in table 2. The total goitre rate according to palpation ranged from 2.4% in Luhe to 5. 1% in Xuyi, and the median urinary iodine concentrations were above 250 mg/L in all counties. The frequency distribution of iodine contents in 6,897 household salt samples analysed by titration is presented in figure 3. Almost 60% of salt iodine concentrations were between 20 and 40 mg/kg, and the large majority were between 20 and 70 mg/kg.
Provincial verification
Table 3 shows the results obtained by the provincial verification team. The total goitre rate according to ultrasonography ranged from 3.0% in Gaoqun to 6.3% in Xuyi, with an average of 3.6%. The urinary iodine concentration of 246 mg/L found in Jurong was the lowest median value, whereas in the other counties the urinary iodine was above 250 mg/L. The proportion of adequate salt iodine levels was above 90% in all counties.
Table 1. Median urinary iodine excretion (UI)(mg/L) and total goitre rate (TGR)(%) during 1983-1997 in nine counties of Jiangsu Province
|
|
1983a |
1985a |
1988-89a |
1992b |
1995b |
1997b |
||||||
|
County |
UI |
TGR |
UI |
TGR |
UI |
TGR |
UI |
TGR |
UI |
TGR |
UI |
TGR |
|
Gaoqun |
65 |
37.1 |
102 |
35.7 |
168 |
18.5 |
251 |
13.6 |
463 |
8.2 |
670 |
2.6 |
|
Jiangning |
79 |
45.3 |
126 |
42.2 |
245 |
19.7 |
324 |
15.4 |
268 |
9.7 |
322 |
2.8 |
|
Jiangpu |
69 |
39.8 |
106 |
39.5 |
236 |
18.6 |
220 |
14.5 |
196 |
8.6 |
358 |
4.7 |
|
Jintan |
80 |
40.4 |
143 |
39.9 |
255 |
17.6 |
216 |
13.3 |
327 |
7.5 |
339 |
4.5 |
|
Jurong |
69 |
42.4 |
104 |
41.5 |
174 |
19.2 |
169 |
15.3 |
362 |
9.4 |
257 |
3.8 |
|
Lishui |
68 |
38.2 |
96 |
37.5 |
196 |
18.5 |
263 |
14.2 |
330 |
8.6 |
318 |
4.9 |
|
Liyang |
64 |
45.8 |
155 |
44.5 |
357 |
19.8 |
452 |
15.6 |
362 |
9.3 |
346 |
4.8 |
|
Luhe |
69 |
41.4 |
99 |
39.7 |
216 |
17.6 |
224 |
14.4 |
241 |
9.4 |
363 |
2.4 |
|
Xuyi |
65 |
43.9 |
89 |
44.3 |
152 |
20.3 |
152 |
18.7 |
415 |
10.3 |
420 |
5.1 |
FIG. 2. Median urinary iodine concentration (UI) and total goitre rate (TGR) in nine counties during 1983-1997
In Jiangsu Province, as in other areas of China and the world, iodization of food-grade salt is the main measure to prevent the public health consequences of iodine deficiency. As evident from the prevalence of goitre in more than 25% of the schoolchildren during surveys in the early 1980s, the population did not obtain sufficient iodine from foods grown indigenously. The low iodine content in drinking water indicated that the iodine deficit was of environmental origin. It also appeared that the nine counties presently under review were the most severely affected. If elimination of iodine-deficiency disorders by salt iodization could be accomplished in these counties, its achievement in other parts of the province, where iodine deficiency was milder, was considered to be less problematic.
The combined population of the nine counties is 5 million, and the geography is hilly and mountainous. Since 1985 the salt-iodization efforts by counties have formed part of an overall strategy to ameliorate iodine deficiency in the population, and prior to 1997 oral iodized oil was distributed annually by health workers to high-risk groups of schoolchildren and women of child-bearing age. Public health surveillance of salt iodine levels and population indicators of iodine-deficiency disorders was also part of the programme from its inception.
The results from the province- and county-based surveillance system indicated that the nine counties have made progress continuously during the past 12 years in supplying iodized salt and reducing iodine-deficiency disorders. The median urinary iodine concentration of the population has remained above 100 mg/L in each county since 1985, and the total goitre rate decreased steadily from above 40% in 1983 to below 5% in 1997. Although the use of iodized oil may have contributed to the urinary iodine improvement, the extent of its contribution is unknown. From the observations it is clear, however, that the use of iodized oil should be discontinued.
Table 2. Salt iodine and population indicators of iodine-deficiency disorders in nine counties of Jiangsu Province, 1997: Results of counties’ self- evaluation
|
|
TGR (%) |
UI (mg/L) |
Salt iodine adequacy |
||||
|
County |
n |
Palpation |
n |
Median |
Range |
n |
% adequacy |
|
Gaoqun |
1,200 |
2.6 |
360 |
670 |
100-2,500 |
750 |
94 |
|
Jiangning |
1,200 |
2.8 |
360 |
322 |
25-3,881 |
897 |
94 |
|
Jiangpu |
1,200 |
4.7 |
360 |
358 |
103-712 |
750 |
93 |
|
Jintan |
1,200 |
4.5 |
360 |
339 |
60-1,540 |
750 |
94 |
|
Jurong |
1,200 |
3.8 |
360 |
257 |
65-3,083 |
750 |
99 |
|
Lishui |
1,200 |
4.9 |
360 |
318 |
130-701 |
750 |
100 |
|
Liyang |
1,200 |
4.8 |
361 |
346 |
34-2,729 |
750 |
100 |
|
Luhe |
1,200 |
2.4 |
360 |
363 |
81-801 |
750 |
100 |
|
Xuyi |
1,200 |
5.1 |
360 |
420 |
24-992 |
750 |
93 |
An effort was made in 1997 by county and provincial authorities to verify the results obtained from surveillance, including the collection of evidence about whether iodine-deficiency disorders had been eliminated in these counties. The design included the collection of salt iodine and population indicators of iodine-deficiency disorders by county officials, complemented by special independent verification of the data by a multisectoral provincial team. Overall, the results obtained by the counties and the provincial team satisfy the criteria recommended by an international expert group [7]. At least 90% of the household salt brought from home for testing at school by a random selection of schoolchildren had >20 ppm iodine, and the total goitre rate in schoolchildren according to palpation was 3.9% for all counties combined. The total goitre rate according to ultrasound was 3.6% on average for all counties. The true prevalence is probably less, however, because the early study [11] is now known to have overestimated goitre status [12]. It is concluded, therefore, that iodine -deficiency disorders in the nine counties of Jiangsu have been eliminated as a public health problem. This means that the consequences of iodine deficiency, such as new cases of endemic cretinism and mental retardation due to iodine deficiency in utero, are extremely rare or nonexistent.
The provincial team concluded from their review of salt production and supply and iodine information-management systems that the mechanism of salt iodization, distribution, and monitoring established in the nine counties was potentially sustainable. At the same time, it must be understood that the iodine deficit of the environment will not be improved by introducing iodine into the food supply. It should be kept in mind that in some countries, after iodine deficiency had been controlled, iodine- deficiency disorders reemerged when governmental, industrial, and popular support for the programme decreased [13]. It was recommended, therefore, that the efforts to maintain regular monitoring of iodized salt and surveillance of the prevalence of iodine-deficiency disorders should be continued.
Table 3. Salt iodine and population indicators of iodine-deficiency disorders in nine counties of Jiangsu Province, 1997: Results of provincial verification
|
|
TGR (%) |
UI (mg/L) |
Salt iodine adequacy |
|||||
|
County |
n |
Palpation |
Ultrasound |
n |
Median |
Range |
n |
% adequacy |
|
Gaoqun |
400 |
3.0 |
3.0 |
120 |
630 |
100-1,030 |
124 |
96 |
|
Jiangning |
400 |
3.3 |
4.5 |
124 |
436 |
25-3,881 |
322 |
91 |
|
Jiangpu |
400 |
2.8 |
3.3 |
120 |
358 |
101-708 |
125 |
98 |
|
Jintan |
400 |
3.3 |
3.5 |
120 |
739 |
39-1,244 |
129 |
100 |
|
Jurong |
400 |
3.0 |
3.5 |
118 |
246 |
60-809 |
125 |
100 |
|
Lishui |
400 |
3.3 |
5.0 |
120 |
309 |
128-578 |
125 |
100 |
|
Liyang |
400 |
3.5 |
4.0 |
120 |
290 |
23-3,879 |
125 |
96 |
|
Luhe |
400 |
3.0 |
4.5 |
121 |
525 |
86-1,028 |
127 |
94 |
|
Xuyi |
400 |
5.0 |
6.3 |
120 |
427 |
40-976 |
122 |
99 |
The elimination of iodine-deficiency disorders from nine counties in Jiangsu Province is a small initial success in accomplishing the national mission launched in 1993 to eliminate iodine-deficiency disorders in China. The approach and methodology applied in this survey may serve as an example for other parts of China as to how the status of iodine- deficiency disorders in a population could be assessed and conclusions drawn to preserve the success of iodine -deficiency disorders elimination, once achieved.
Acknowledgments
The evaluation mission was supported by the Office for Endemic Disease Control, Jiangsu Provincial Government. We thank the governments and salt producers in the nine counties. We are grateful to Dr. P. H. Wang, Mr. X. X. Yang, Mr. Z. G. Chen, Mr. D. M. Zhang, Dr. T. Y. He, Mr. T. Z. Zhang, and others for their involvement in data and sample collection, and laboratory analysis. We also thank the children and their families for their participation in the surveys.
1. Delange F. The disorders induced by iodine deficiency. Thyroid 1994;4:107-28.
2. UNICEF. First call for children: world declaration and plan of action. World summit for children. New York: UNICEF, 1990.
3. World Health Organization/UNICEF. World summit for children mid-decade goal: iodine deficiency disorders. Document JCHPSS/94/2.7. Geneva: WHO, 1993.
4. UNICEF. The state of the world’s children 1998. New York: Oxford University Press, 1998:54.
5. Zheng JD, Yang XX. Investigation of endemic goiter in Jiangsu Province. Jiangsu J Med Pharmacy 1986;2:86-9.
6. Zhao JK Cross-sectional survey of iodized salt in Jiangsu. Jiangsu J Prevent Med 1997;3(2):130-2.
7. World Health Organization/UNICEF/International Council for the Control of Iodine-Deficiency Disorders. Indicators for assessing iodine deficiency disorders and the control through salt iodization. WHO/NUT/94.6. Geneva: WHO, 1994.
8. Brunn J, Block U, Ruf G, Bos I, Kunze WP, Scriba PC. Volumetric analysis of thyroid lobes by real-time ultrasound. Deutsche Medizinische Wochenschrift 1981;106:1338-40.
9. Dunn JT, Crutchfield HE, Gutekunst R, Dunn AD. Two simple methods for measuring iodine in urine. Thyroid 1993;3:119-23.
10. Sullivan KM, Houston R, Gorstein J, Cervinskas J. Monitoring universal salt iodization programmes (UNICEF/PAMM/MI/ICCIDD/WHO). Atlanta, Ga, USA, and Ottawa, Canada: PAMM and MI, 1995.
11. Gutekunst R, Martin-Teichert H. Requirements for goiter surveys and the determination of thyroid size. In: Delange F, Dunn JT, Glinoer D, eds. Iodine deficiency in Europe. New York: Plenum Press, 1993:109-15.
12. Delange F, Benker G, Caron P, Eber O, Ott W, Peter F, Podoba J, Simescu M, Szybinsky Z, Vertongen F, Vitti P, Wiersinga W, Zamrazil V. Thyroid volume and urinary iodine in European schoolchildren: standardization of values for assessment of iodine deficiency. Eur J Endocrinol 1997;136:180-7.
13. Freire W, Dunn IT, Pretell EA, Van de Haar F, Alnwick DA, Rivadeneira MA, Lechtig A. Report of an external review of the Bolivia IDD control programme: virtual elimination of iodine deficiency disorders achieved in Bolivia. La Paz, Bolivia: UNICEF, 1996.
14. Stanbury JB, Ermans AE, Bourdoux P, Todd C, Oken E, Tonglet R, Vodor G, Braverman LE, Medeiros-Neto G. Iodine-induced hyperthyroidism: occurrence and epidemiology. Thyroid 1998;8:83-100.
15. World Health Organization/UNICEF/International Council for the Control of Iodine-Deficiency Disorders. joint consultation. Review of findings from 7-country study in Africa on levels of salt iodization in relation to iodine deficiency disorders, including iodine-induced hyperthyroidism. Document WHO/AFRO/NUT/97.2. Brazzaville, Congo: WHO, 1997:27-29.
![]()
![]()
![]()
{kind=link}